This information is designed only to help patients talk with their physicians about Trigeminal Neuralgia (TN) and is not intended to provide treatment guidelines. There are some excellent patient support group web sites that you might wish to review.
I had the opportunity to give a lecture to the Trigeminal Neuralgia Association of Canada (TNAC) on Saturday March 30, 2013 via a Webinar. Most of that lecture is summarized below in the following paragraphs.
Introduction
This painful facial condition has been described in the medical literature for over a thousand years. There is some controversy as to who first described the symptoms. The Greek physician Aretaeus of Cappodocia wrote a series of medical texts (circa 150 AD). Book I was “On the causes and symptoms of chronic disease” and in Chapter II, he described a condition where,
“the pain does not pass this limit, but remains in the half of the head. This is called Heterocrania, an illness by no means mild, even though it intermits, and although it appears to be slight. For if at any time it set in acutely, it occasions unseemly and dreadful symptoms; spasm”
Aretaeus of Cappodocia (circa 150AD)
One could argue that he was describing the much more common condition of migraine – hence the controversy in the medical literature. A more convincing description comes from the Arab scholar Ibn Sina (980-1037) who was known to the Western world by his Latin name Avicenna. He described the following,
“Leqvet is a type of organic disease affecting one side of the face, [paralysis or spasm]…The other sign of the disease is pain in the face. The skin is dry and there are convulsions on that side of the face.”
Ibn Sina (980 – 1037)
There were two conditions described. The first was facial palsy (a paralysis of one side of the face) and the second was likely trigeminal neuralgia. In my reading of the literature, the first definite description of trigeminal neuralgia appeared in the eulogy of Dr. Johannes Bausch (1605-1665). Dr. Bausch was the first president and founding member of the German Academy of Sciences Leopoldina (the oldest continuously existing learned society in the world). He died of trigeminal neuralgia! His eulogy was published in the local newspaper and is an excellent description of some of poor Dr. Bausch’s symptoms,
“…a sharp, shooting pain in his right maxilla that came on suddenly like a bolt of lightening, varying in intensity, leaving him unable to speak or eat solid food.
“In the fall of 1665, the pain disappeared, only to return early that same winter. The pain was so intense that it forced him to remain bedridden. He eventually died of malnutrition because his dietary intake was limited by the excruciating pain.”
Johann Bausch (1605-1655)
The condition was described in a medical book by a French physician, Nicolaus Andre, in 1756. He called it “tic douloureux”. This is a term you might still hear today. Andre was taken by the fact that patients always contracted their face when they had the pain – hence the ‘tic’ and he believed this was part of the disease. We know that the ‘tic’ or facial grimace is just a reaction to the pain. There is no forced contraction of the face with the pain. Patients are able to keep their face motionless during the pain if they want. The knowledge that there were separate nerves in the face – one controlling facial movement and another controlling facial sensation was not known when Andre was working and it would not be discovered until Sir Charles Bell published his text on the nervous system in 1811. Another British physician, John Fothergill, described trigeminal neuralgia very well in his paper “Of a painful affliction of the face’ in 1773. He wrote,
“The pain comes suddenly and is excruciating; it lasts but a short time…Eating, talking or the gentlest touch of a handkerchief will sometimes bring on the pain”
In the UK, trigeminal neuralgia is still sometimes known as Fothergill’s disease. These historical accounts of trigeminal neuralgia are interesting because they describe the disease so well. Readers will be horrified to know that one of my patients reported that she almost starved to death before the diagnosis was made and she received treatment in 2012. History repeats!
Trigeminal neuralgia will occur in about 5 new patients for every 100,000 people each year. It can occur at any age but is far more common as you get older. It is particularly common in multiple sclerosis (MS) where approximately 2% get it (that would be 2,000 patients for every 100,000 with MS)-that is very much more common than the general population.
The current consensus is that TN is caused by demyelination of the trigeminal nerve. The trigeminal nerve carries information about what is touching the face back to the brain. This information is carried in little nerve fibers that are insulated from each other by myelin (like wires are insulated). If the insulation is lost (demyelination), then the nerves can “short-circuit”. Signals coming down one nerve fiber can spread to many nerve fibers and barrage the brain with signals (felt as the TN pain). The trigeminal nerve can lose myelin in certain diseases such as multiple sclerosis or more commonly by constant pressure from an abnormally located artery. The trigeminal nerve has three branches (hence “tri”-geminal) which join together as the nerves enter the skull. The first branch (ophthalmic or V1) controls sensation to the forehead. The second branch (maxillary or V2) covers sensation from below the eye to the corner of the lip. The third branch (mandibular or V3) covers sensation below the corner of the lip to the angle of the jaw. The pain of TN is often felt in a single territory (usually V2 or V3) but in severe cases can include all three division.
Diagnosis
The diagnosis of trigeminal neuralgia is made almost exclusively by the history or description of the problem.
Symptoms are described as brief sudden intense pains on one side of the face. The pain is typically sharp or electrical and last for a few seconds or a minute. In between ‘shots’ or ‘bolts’ of pain, the patient is pain free (until another shot comes). It is important to note that initially this is an intermittent pain. There are completely painfree intervals between attacks. It is very suggestive of trigeminal neuralgia if the pain can be triggered by lightly touching the skin. This usually occurs when the patient is in the middle of a bad bout of neuralgia. Other common triggers include brushing the teeth, eating or moving the jaw – talking or chewing.
The pain can be accompanied by autonomic features (i.e. swelling or redness of the face, tearing of the eye or increased saliva).
Over the years, the pain is expected to come and go. Remissions can last for years initially but usually get shorter over time. Relapses (when the pain comes back) tend to get more and more severe over the years.
Occasionally, if the pain has been around for a longtime, patients can develop a constant pain in the region of their face usually described as a burning sensation.
The pain of trigeminal neuralgia is expected to improve following appropriate medical treatment (i.e. following Carbamazepine or Neurontin).
The condition is often confused with dental pain and many patients have teeth extracted before the diagnosis is made! To be fare to our dental colleagues, the very first pain of trigeminal neuralgia (before it gets severe) can be described as a toothache. This is sometimes called ‘pre-neuralgia’.
An important aid in the diagnosis of trigeminal neuralgia is a MRI scan. This scan should be ordered to rule out MS (i.e. FLAIR sequence to look for white matter lesions) and to detect a vascular compression of the trigeminal nerve (i.e. FIESTA or CISS sequence). The interpretation of these images can be difficult especially if one is not familiar with what to look for. I have had a number of patients delayed in their surgical consultation because the MRI was read as ‘normal’ even though there was a clear example of a vascular compression. The condition is rare enough that some radiologists may not have seen any examples of vascualr compression.
MRI showing MS
This MRI shows multiple bright white lesions extending at right angles from the peri-ventricular area. It is an example of the imaging seen in multiple sclerosis (MS).
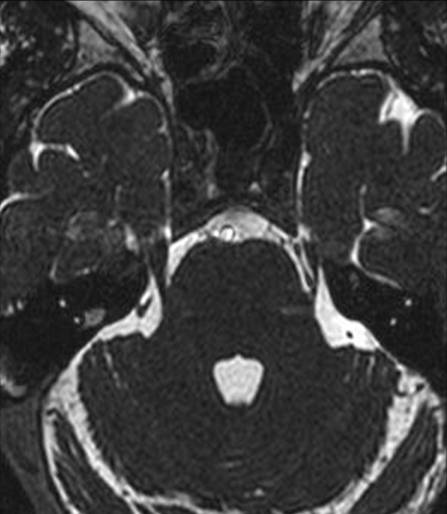
MRI showing Vascular Compression
This MRI shows the left and right trigeminal nerves entering the brainstem on either side of the pons. The nerve on your right (actually the patient’s left) is compressed by a loop of a blood vessel which pushes the nerve out and away from the brainstem. The blood vessel is seen almost at the bottom of its loop so you see a vessel (in front) heading downwards and the same vessel (at the back) is seen as it is heading back up.
Treatment
The treatment of trigeminal neuralgia has a long history. The first (unsuccessful) medical treatment was provided by the famous British philosopher and physician John Locke to the wife of the British ambassador to France in 1677 – he gave her laxatives! The first successful medication was Dilantin introduced in 1942. The first neurosurgeon, Sir Victor Horsley, tried cutting the nerve and by the 1920’s neurosurgeons began routinely treating trigeminal neuralgia by cutting portions of the nerve. It became clear that the nerve was often compressed by a blood vessel when surgeons explored the nerve in preparation to cut it. The suggestion was then advanced that the condition could be treated by decompressing the nerve instead of cutting it and the Microvascular Decompression operation was born.
Medical Treatments
Most patients with TN can be treated with medications designed to dampen nerve signals. Medications such as Tegretol, Dilantin, or Neurontin (used commonly to prevent seizures in epileptics) can reduce or eliminate the pain. Each medication can produce side effects of tiredness, dizziness, and slowing of thinking in higher doses. Surgery is reserved for two groups of patients:
1. patients who can not control their pain with pills
2. patients who can not tolerate the side-effects of the pills needed to control their pain
Rarely is surgery an emergency – for patients who can not swallow and are therefore dehydrated (remember Dr. Bausch died of this condition) or unable to take their neuralgia pills.
The picture below is of a drawing by Leonardo da Vinci from approximately 1485. The anguish on the man’s face reminded me of the pain of trigeminal neuralgia.
 Parkinson's Disease
Parkinson's Disease Tremor
Tremor Dystonia
Dystonia Trigeminal Neuralgia
Trigeminal Neuralgia Hemifacial Spasm
Hemifacial Spasm Multiple Sclerosis
Multiple Sclerosis DBS Clinic
DBS Clinic Dental Neuralgia or Anesthesia Dolorosa
Dental Neuralgia or Anesthesia Dolorosa Glossopharyngeal Neuralgia
Glossopharyngeal Neuralgia Hemi-Laryngopharyngeal Spasm (HELPS syndrome)
Hemi-Laryngopharyngeal Spasm (HELPS syndrome) Information for Physicians
Information for Physicians International Patients
International Patients Post Herpetic Neuralgia (of the face)
Post Herpetic Neuralgia (of the face) Spasmodic Dysphonia
Spasmodic Dysphonia The Tenth Nerve
The Tenth Nerve VANCOUVER syndrome
VANCOUVER syndrome